
Use medicine balls to develop upper-body strength, power, and elasticity through a variety of passes and throws. Throwing the medicine ball back and forth with a partner is a productive and fun activity. When a partner isn’t available, throw the medicine ball against a solid wall structure to develop athletic upper-body qualities. The decision to use partner throws rather than the wall throws depends on availability of equipment and facilities as well as the objectives of the training session.
Selecting an appropriate medicine ball for chosen activities is an important step in the process. The ball must be constructed of a material that is easy to grip and also provides some degree of cushioning, or give. A ball that is too hard is not only harder to catch but also very stressful on the hands over numerous repetitions. A ball that is too soft may not provide enough bounce for rebounding against a wall. Smaller medicine balls may be difficult to catch, but larger medicine balls can be difficult to throw. Finally, the weight of the medicine ball must be appropriate for you and your chosen exercise. When in doubt, always opt for a slightly lighter ball for safety and preservation of movement quality.
In this week’s technical feature, we share a series of different medicine ball throws from Plyometric Anatomy by Derek Hansen and Steve Kennelly.
Medicine Throws
Exercise 1: Underhand Vertical Squat Throw
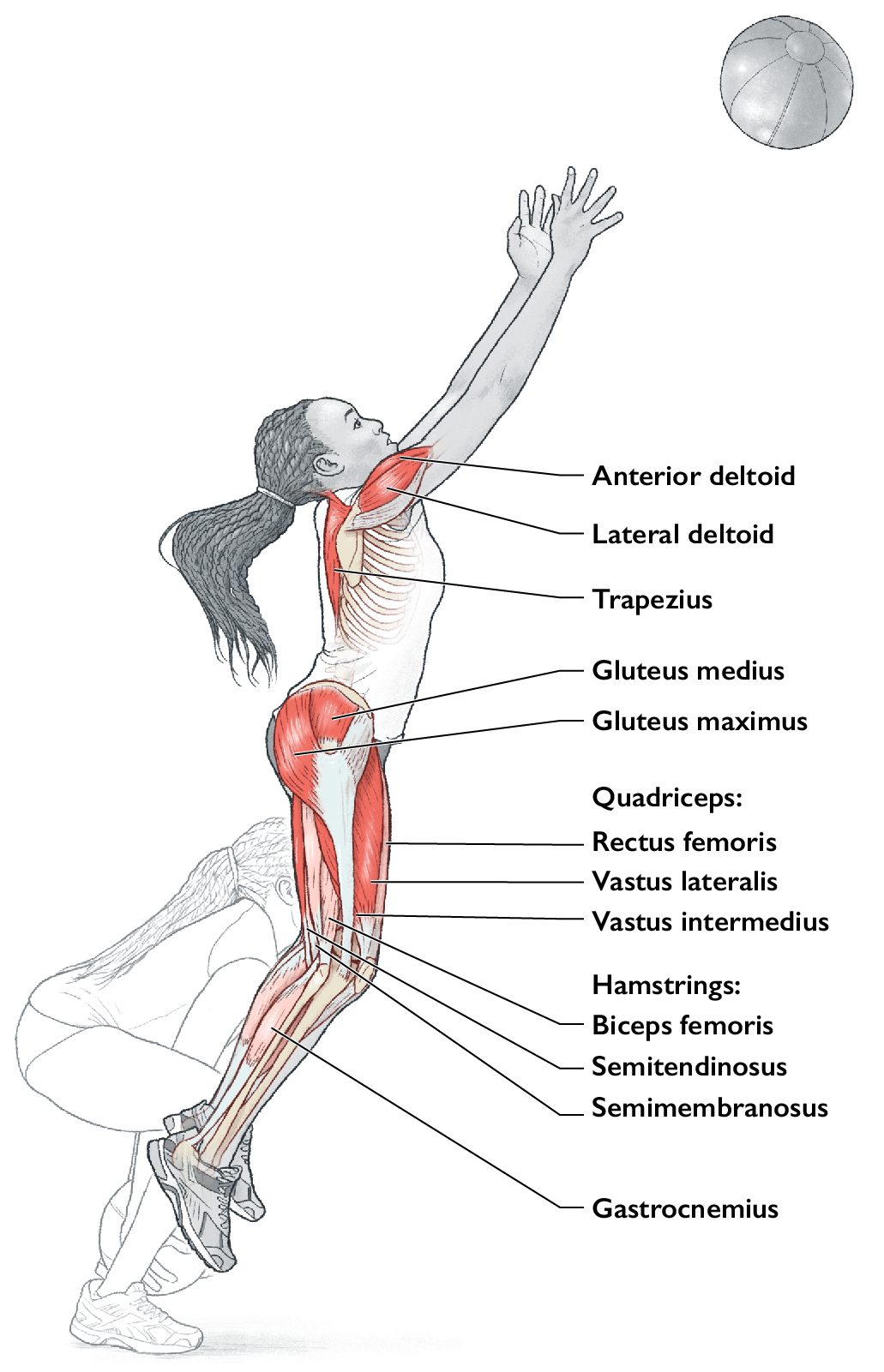
Execution
- Stand in a tall posture and hold the medicine ball in front of the body at waist height
- Descend into a low squat, keeping the torso upright, arms extended and ball in front of the body to generate additional force from the lower body
- Extend vertically from the knees and hips, accelerating the body upward similar to a squat jump movement and maintain an extended arm position through the jump; if enough force is generated during the throw, it is common for the feet to leave the ground
- At the top of the squat, pull the medicine ball powerfully upward along the body for maximum height on the throw; the trajectory of the throw can be vertical or slightly forward, particularly if passing to a partner
- The body can extend off the floor at the end of the throw, particularly if it is a powerful effort; make sure the ball does not hit you when it falls back down
Muscles involved
Primary: trapezius, lateral deltoid, anterior deltoid, gluteus maximus, gluteus medius, semitendinosus, vastus lateralis, vastus medialis, vastus intermedius.
Secondary: gastrocnemius, biceps femoris, semimembranosus, rectus femoris.
Exercise notes
The Underhand Vertical Squat Throw can be an explosive exercise at maximal intensity or a general strength activity performed at submaximal intensity. The maximal heave throw develops upper-body pulling power for sports such as rowing and wrestling. The lower-body contributions can be helpful for overall starting strength and vertical jumping ability. As with many throws, the combination of lower-body power at the beginning of the movement and upper-body speed toward the end of the throw produces a high-velocity performance that launches the ball for maximum distance. Launch the ball along the front of the body in a vertical path and for maximal efforts perform 6 to 8 repetitions in each set. For submaximal throws, perform 8 to 15 repetitions in each set. When you cannot perform Olympic weightlifting movements, maximal heave throws for height are a viable substitute for developing vertical power.
Exercise 2: Split-Stance Scoop Throw
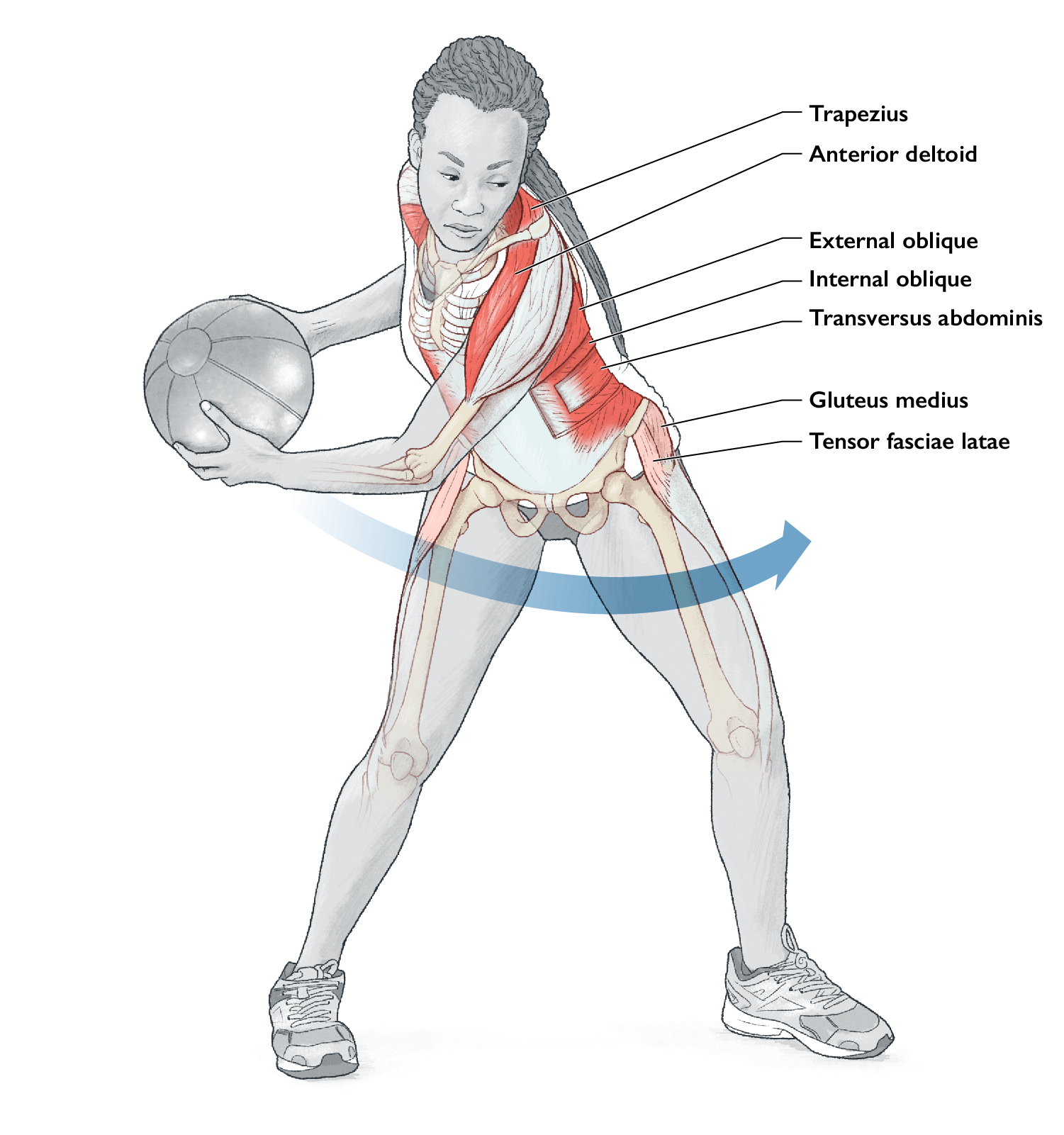
Execution
- Start in a moderate split stance with the feet approximately 12-16 inches (30-40 cm) apart from heel to toe (the stance width can be similar to the width of the shoulders) and maintain an upright posture, holding the medicine ball to one side of the body with the arms extended
- Draw the medicine ball back past the rear hip and then throw the ball forcefully in a powerful underhand scoop throw to a partner or against a solid wall; the partner returns the ball to the height of the mid-section (if using a wall throw, stand close enough to the wall to have the ball returned to waist height with a powerful throw)
- Repeat the throw in a rhythmic fashion on one side, then switch to the other side for the next set
Muscles involved
Primary: trapezius, anterior deltoid, transversus abdominis, internal oblique, external oblique, multifidus.
Secondary: gluteus medius, erector spinae (iliocostalis, longissimus, spinalis), tensor fasciae latae.
Exercise notes
You can do this exercise as a rhythmic set of circuit passes for general strength and fitness or as a more explosive throw to develop rotational power. Establish a good base of support in the split stance.
Variation – Drop Split into Scoop Throw
Stand tall and drop into a split position with the front thigh parallel to the ground, before the scoop throw for a more dynamic version of this exercise. The drop into a split stance loads the lower body and uses elastic strength properties before a powerful scoop throw. Make sure not to split into a stance so deep that the knee of the rear leg contacts the ground. These types of dynamic movements into throws are useful for sports that require reactive footwork in order to achieve a better position for receiving a ball, such as in volleyball, tennis, squash, and badminton.
Exercise 3: Kneeling Lateral Underhand Pass
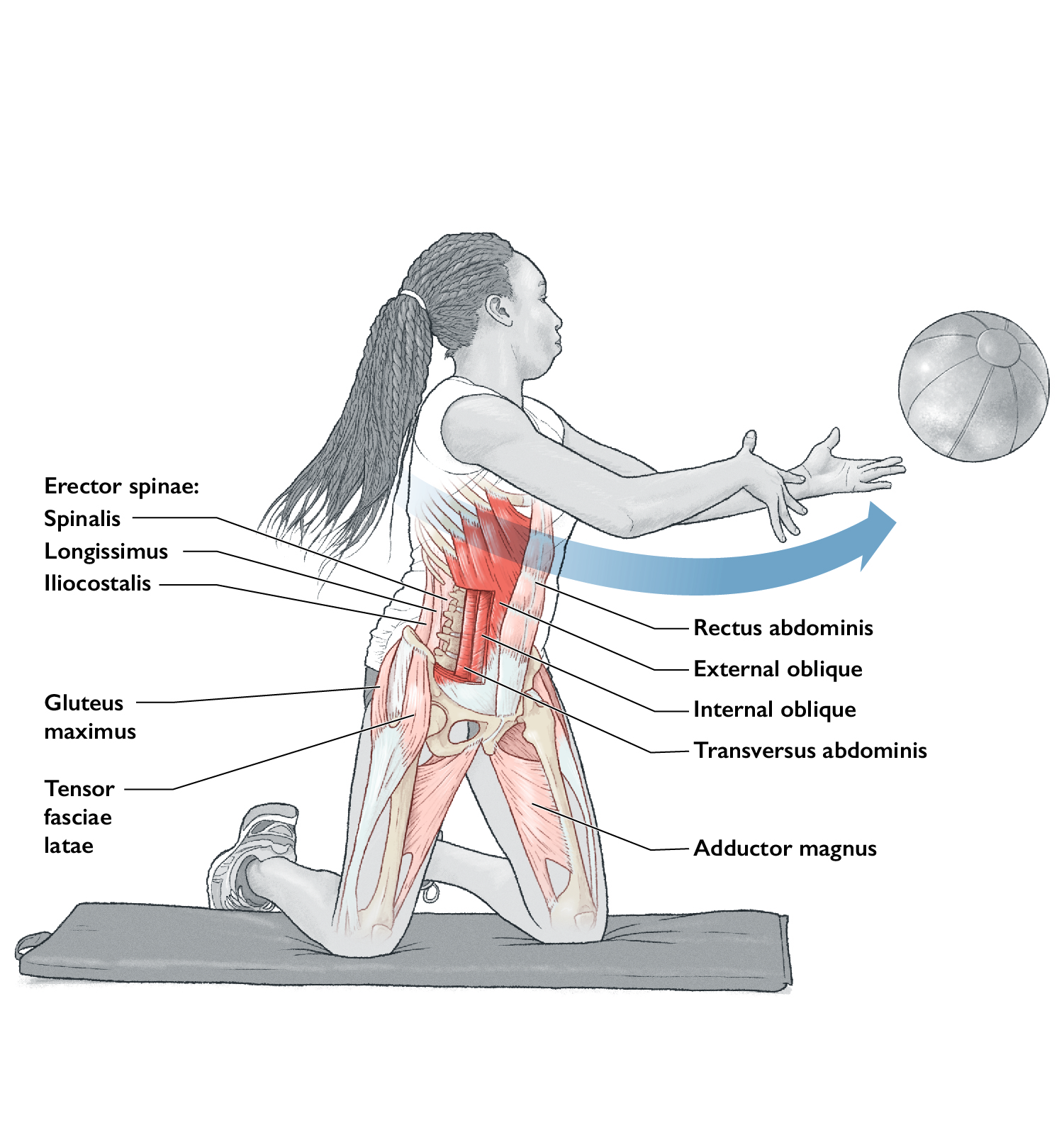
Execution
- Get into a kneeling position perpendicular to the direction of the throw and hold the medicine ball in front of the body at waist height (the throw can be to a partner or against a solid wall); kneel on a soft surface or with an appropriate pad or exercise mat beneath the knees
- Draw the ball away from the direction of the throw, rotating the shoulders relative to the hips to pre-stretch the muscles of the core
- Throw the medicine ball powerfully across the body with the path of the ball close to the abdomen; follow through with the arms and shoulders on the release of the ball
- When receiving the ball from a partner or a rebound off the wall, catch the ball in advance of the body and rotate back to the far side of the body to prepare for the next throw
- Perform on one side of the body in one set, then switch to the other side for the next set
Muscles involved
Primary: transversus abdominis, internal oblique, external oblique, multifidus.
Secondary: rectus abdominis, erector spinae (iliocostalis, longissimus, spinalis), tensor fasciae latae, adductor magnus, gluteus maximus.
Exercise notes
A lateral pass from the knees requires greater rotation and mobility through the core to achieve appropriate range of motion in both the gather and delivery phases than a standing lateral pass. The pull of the medicine ball across the body should be powerful, making use of the force-generating abilities of both the upper body and core. Perform quick passes close to a wall or partner, or pass in a forceful manner with greater distance required on each throw.
Variation – Kneeling Rotational Pass Behind
An even greater range of motion is required to turn the shoulders to enable a rotating pass behind the body from the kneeling position. A partner stands behind you, slightly off to one side to receive the pass. The return pass from the partner provides additional momentum for the countermovement to the opposite side of the body, generating greater force for individual passes. The rotational passes need not be maximal because the main intent is to achieve greater range of motion through repetitive throws in a strong, rhythmic fashion.
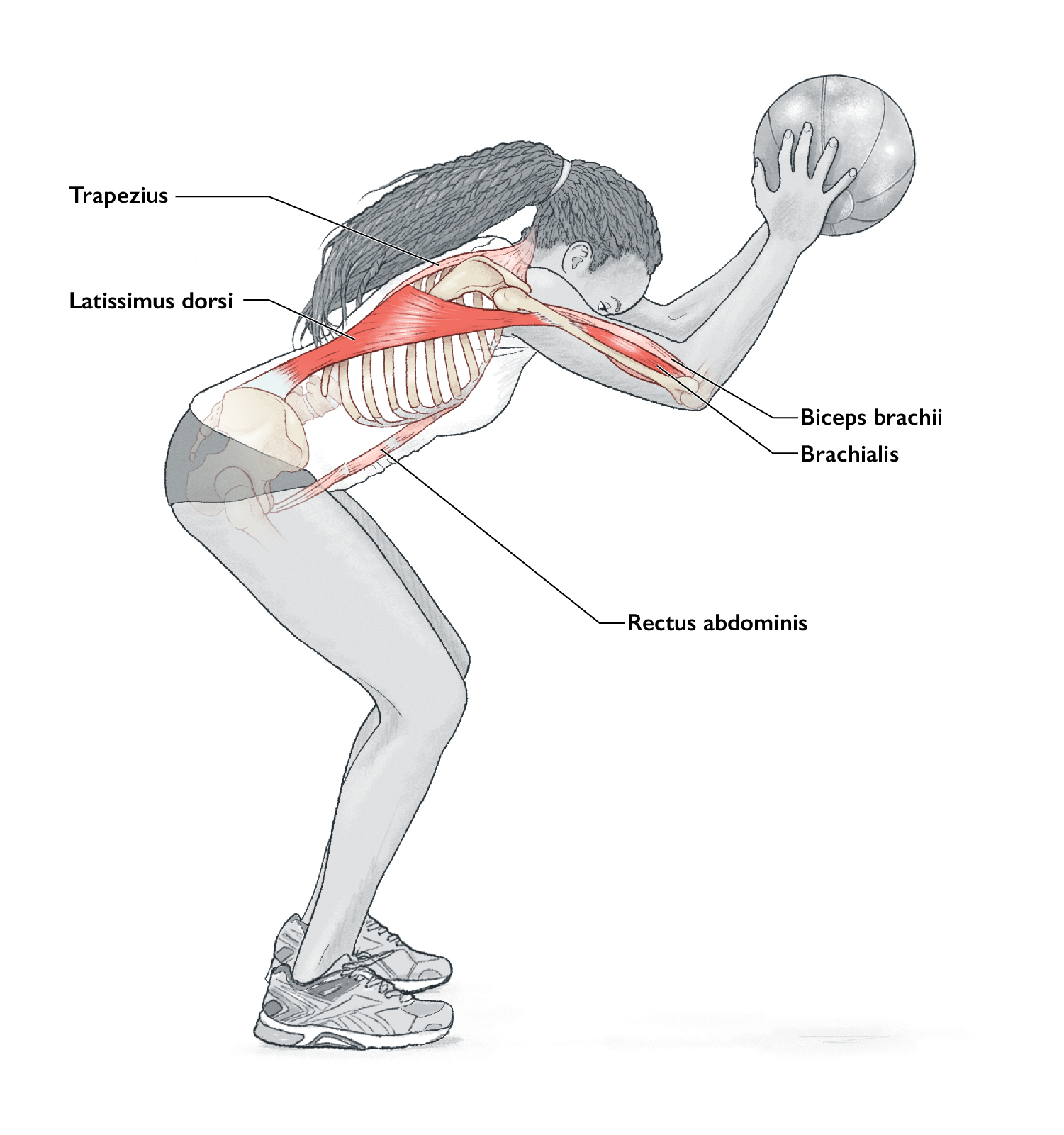
Exercise 4: Kneeling Medicine Ball Overhead Pass
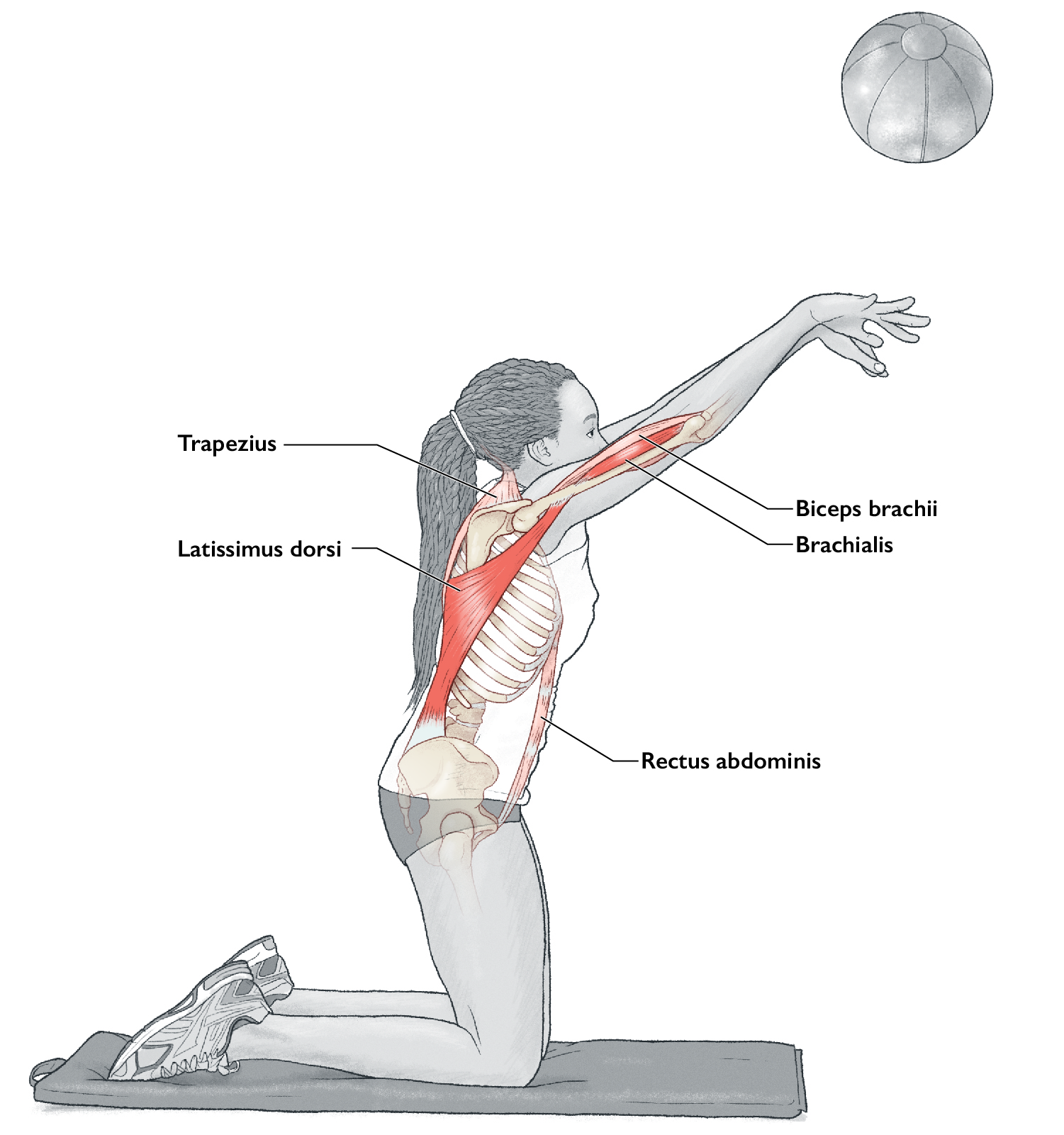
Execution
- Begin the exercise from a bilateral kneeling position on a soft surface
- Draw the medicine ball behind the head and then pass powerfully to a partner or against a firm wall
- Use a lighter medicine ball and a closer distance between yourself and your partner or the wall for easier passes from the kneeling position because throwing from this position places greater stress on the arms and shoulders
- Receive the ball from a partner throw or wall rebound at the point of initial release; once the catch is made above the head, allow the ball to draw back behind the head to load the primary muscles to stretch in preparation for the next throw
- Maintain a firm posture throughout the exercise with a strong, stable stance from the kneeling position
Muscles involved
Primary: latissimus dorsi, brachialis.
Secondary: rectus abdominis, trapezius, biceps brachii.
Exercise notes
A Kneeling Medicine Ball Overhead Pass places a greater load on the upper body and core than a standing pass. Shorter passes with lower throw velocities are to be expected from the kneeling position than from the standing position, where more muscles and joints are involved in the summation of force for the throwing action.
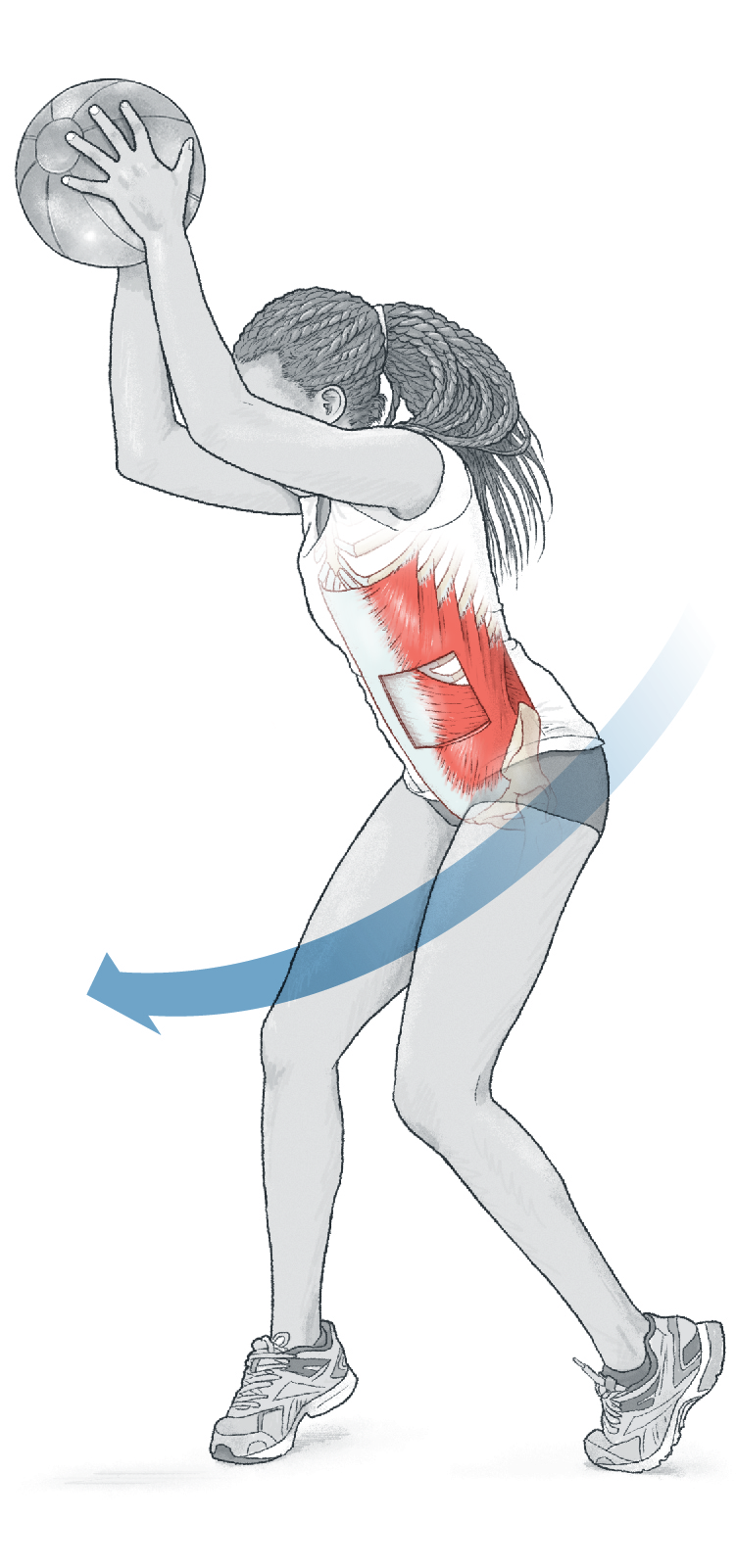
Variation – Falling Kneeling Medicine Ball Overhead Pass
Falling forward as part of the throwing motion from the knees adds force and velocity to the medicine ball throw. Practice under submaximal conditions to ensure you can complete the throw and safely slow your fall to the ground by using your arms.
Exercise 5: Downward Slam Throw
Execution
- Stand tall with feet hip-width apart and hold the medicine ball directly overhead with the arms fully extended
- Initiate the movement by bending forward at the waist and dropping the torso powerfully to develop tension in the arms and shoulders
- Drive the ball down to the floor with the arms extended and target a spot on the floor that is at least 12 inches away from the feet to ensure the ball does not bounce back up into your face
- Repeat the downward throws methodically, not rushing from repetition to repetition
Muscles involved
Primary: latissimus dorsi, brachialis.
Secondary: rectus abdominis, iliopsoas, trapezius, biceps brachii.
Exercise notes
The Downward Slam Throw with a medicine ball is a dynamic exercise that targets anterior musculature required for powerful swimming strokes and other sporting activities that involve throwing or grappling. The motion begins with the core musculature and is delivered by the arms. Because the throwing motion can be very stressful for the shoulders, select an appropriate medicine ball weight so you are not overloaded. Additionally, shorter repetition ranges are advisable for initial sessions to ensure technique is optimised before higher volumes of work are incorporated.
Variation – Rotational Downward Slam Throw
You can perform a rotational version of this exercise so that you slam the medicine ball down to either side of the body. The exercise is set up similar to a standard Downward Slam Throw, but you begin to turn to one side once you initiate the downward motion. This variation places a greater emphasis on the oblique muscles of the core.
Like to get more content like this without having to search? Sign up for the free FitPro newsletter delivered to your inbox bi-weekly.
This article is an excerpt from Plyometric Anatomy by Derek Hansen and Steve Kennelly and reproduced with permission. The exercises can be found between pages 162-183. Visit: humankinetics.com/products/all-products/plyometric-anatomy
Where next? Box jump variations
Have you got a question about the article? Email: [email protected] and let us know what technical topics you would like to read in future FitPro newsletters.





